Colon cancer is cancer that forms in the
tissues of the colon (the longest part of
the large intestine). Most colon
cancers are adenocarcinomas (cancers that begin in cells
that make and release mucus and other fluids).
Rectal cancer is cancer that forms in the tissues of the rectum (the last several inches of the large intestine before the anus).
Worldwide, cancer of the colon and rectum (known collectively as colorectal
cancer) is the third leading cause of cancer in males and the fourth
leading cause of cancer in females. The frequency of colorectal cancer varies
regionally. It is common in the Western world, and has been traditionally
rare in Asia and Africa. In countries where people have adopted western
diets, rich in animal fat, the incidence of colorectal cancer is increasing.
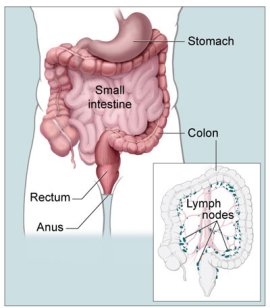
Colon and rectum
The colon and rectum are parts of the gastrointestinal
(GI) tract. They form a long, muscular tube called the large intestine
or large bowel). The colon is the first 4 to 5 ft of the large intestine,
and the rectum is the last several inches.
Partly digested food enters the colon from the small
intestine. The colon removes water and nutrients from the food and turns
the rest into waste (feces or stool). The
waste passes from the colon into the rectum and then out of the body through
the anus.
Who is at risk?
No one knows the exact causes of colorectal cancer. Doctors often cannot
explain why one person develops this disease and another does not. However,
it is clear that colorectal cancer is not contagious. No one can catch this
disease from another person.
Research has shown that people with certain risk factors are more likely
than others to develop colorectal cancer. A risk factor is something that
may increase the chance of developing a disease.
Studies have found the following risk factors for colorectal cancer:
Age over 50. Colorectal cancer is more likely to
occur as people get older. More than 90% of people with this
disease are diagnosed after age 50. The average age at diagnosis is
72.
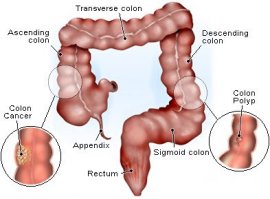
Colorectal polyps. Polyps are growths on the inner wall of the colon or rectum. They are common
in people over age 50. Most polyps are benign (not cancer), but some
polyps (adenomas) can become cancer. Finding and removing polyps may
reduce the risk of colorectal cancer.
Family history of colorectal cancer. Close relatives
(parents, brothers, sisters, or children) of a person with a history
of colorectal cancer are somewhat more likely to develop this disease
themselves, especially if the relative had the cancer at a young age.
If many close relatives have a history of colorectal cancer, the risk
is even greater.
Genetic alterations. Changes in certain genes increase
the risk of colorectal cancer.
-
Hereditary nonpolyposis colon cancer (HNPCC) is the most
common type of inherited (genetic) colorectal cancer. It accounts
for about 2% of all colorectal cancer cases. It is caused
by changes in an HNPCC gene. Most people with an altered HNPCC gene
develop colon cancer, and the average age at diagnosis of colon
cancer is 44.
-
Familial adenomatous polyposis (FAP) is a rare, inherited
condition in which hundreds of polyps form in the colon and rectum.
It is caused by a change in a specific gene called APC. Unless FAP
is treated, it usually leads to colorectal cancer by age 40. FAP
accounts for less than 1% of all colorectal cancer cases.
Family members of people who have HNPCC or FAP can have genetic testing
to check for specific genetic changes. For those who have changes in their
genes, health care providers may suggest ways to try to reduce the risk
of colorectal cancer, or to improve the detection of this disease. For adults
with FAP, the doctor may recommend an operation to remove all or part of
the colon and rectum.
Personal history of cancer. A person who has already
had colorectal cancer may develop colorectal cancer a second time. Also,
women with a history of cancer of the ovary, uterus (endometrium), or breast are at
a somewhat higher risk of developing colorectal cancer.
Ulcerative colitis or Crohn's
disease. A person who has had a condition that causes inflammation of the colon (such as ulcerative colitis or Crohn's disease) for many
years is at increased risk of developing colorectal cancer.
Diet. Studies suggest that diets high in fat (especially
animal fat) and low in calcium, folate, and fiber may increase the risk
of colorectal cancer. Also, some studies suggest that people who eat
a diet very low in fruits and vegetables may have a higher risk of colorectal
cancer. However, results from diet studies do not always agree, and
more research is needed to better understand how diet affects the risk
of colorectal cancer.
Cigarette smoking. A person who smokes cigarettes
may be at increased risk of developing polyps and colorectal cancer.
Because people who have colorectal cancer may develop colorectal cancer
a second time, it is important to have checkups. If you have colorectal
cancer, you also may be concerned that your family members may develop the
disease. People who think they may be at risk should talk to their doctor.
The doctor may be able to suggest ways to reduce the risk and can plan an
appropriate schedule for checkups. See the "Screening" section to learn
more about tests that can find polyps or colorectal cancer.
Screening
Screening tests help your doctor find polyps or cancer before you have symptoms.
Finding and removing polyps may prevent colorectal cancer. Also, treatment
for colorectal cancer is more likely to be effective when the disease is
found early.
To find polyps or early colorectal cancer:
People in their 50s and older should be screened.
People who are at higher-than-average risk of colorectal cancer should
talk with their doctor about whether to have screening tests before
age 50, what tests to have, the benefits and risks of each test, and
how often to schedule appointments.
The following screening tests can be used to detect polyps, cancer, or other
abnormal areas.
Your doctor can explain more about each test:
Fecal occult blood test (FOBT). Sometimes cancers
or polyps bleed, and the FOBT can detect tiny amounts of blood in the
stool. If this test detects blood, other tests are needed to find the
source of the blood. Benign conditions (such as hemorrhoids) also can
cause blood in the stool.
Sigmoidoscopy.
Your doctor checks inside your rectum and the lower part of the colon
with a lighted tube called a sigmoidoscope. If polyps are found, the
doctor removes them. The procedure to remove polyps is called a polypectomy.
Colonoscopy.
Your doctor examines inside the rectum and entire colon using a long,
lighted tube called a colonoscope. Your doctor removes polyps that may
be found.
Double-contrast barium enema. You are given an enema
with a barium solution, and air is pumped into your rectum. Several X-ray pictures are taken
of your colon and rectum. The barium and air help your colon and rectum
show up on the pictures. Polyps or tumors may show up.
Digital rectal exam. A rectal exam is often part
of a routine physical examination. Your doctor inserts a lubricated,
gloved finger into your rectum to feel for abnormal areas.
Virtual colonoscopy. This method is under study.
Signs and symptoms
A common symptom of colorectal cancer is a change in bowel habits. Symptoms
include:
Having diarrhea or constipation
Feeling that your bowel does not empty completely
Finding blood (either bright red or very dark) in your stool
Finding your stools are narrower than usual
Frequently having gas pains or cramps, or feeling full or bloated
Losing weight with no known reason
Feeling very tired all the time
Having nausea or vomiting
Most often, these symptoms are not due to cancer. Other health problems
can cause the same symptoms. Anyone with these symptoms should see a doctor
to be diagnosed and treated as early as possible.
Usually, early cancer does not cause pain. It is important not to wait to
feel pain before seeing a doctor.
Diagnosis
If you have screening test results that suggest cancer or you have symptoms,
your doctor must find out whether they are due to cancer or some other cause.
Your doctor asks about your personal and family medical history and gives
you a physical exam. You may have one or more of the tests described in
the "Screening" section.
If your physical exam and test results do not suggest cancer, your doctor
may decide that no further tests are needed and no treatment is necessary.
However, your doctor may recommend a schedule for checkups.
If tests show an abnormal area (such as a polyp), a biopsy to check for cancer cells may be necessary. Often, the abnormal tissue can
be removed during colonoscopy or sigmoidoscopy. A pathologist checks the
tissue for cancer cells using a microscope.
You may want to ask your doctor these questions before having a biopsy:
How will the biopsy be done?
Will I have to go to the hospital for the biopsy?
How long will it take? Will I be awake? Will it hurt?
Are there any risks? What are the chances of infection or bleeding
after the biopsy?
How long will it take me to recover? When can I resume a normal diet?
How soon will I know the results?
If I do have cancer, who will talk to me about the next steps? When?
Staging the disease
If the biopsy shows that cancer is present, your doctor needs to know the
extent (stage) of the disease to plan the best treatment. The stage is based
on whether the tumor has invaded nearby tissues, whether the cancer has
spread and, if so, to what parts of the body.
Your doctor may order some of the following tests:
Blood tests.
Your doctor checks for carcinoembryonic antigen (CEA) and other substances
in the blood. Some people who have colorectal cancer or other conditions
have a high CEA level.
Colonoscopy. If colonoscopy was not performed for
diagnosis, your doctor checks for abnormal areas along the entire length
of the colon and rectum with a colonoscope.
Endorectal ultrasound.
An ultrasound probe is inserted into your rectum. The probe sends out
sound waves that people cannot hear. The waves bounce off your rectum
and nearby tissues, and a computer uses the echoes to create a picture.
The picture may show how deep a rectal tumor has grown or whether the
cancer has spread to lymph nodes or other nearby tissues.
Chest X-ray.
X-rays of your chest may show whether cancer has spread to your lungs.
CT scan.
An X-ray machine linked to a computer takes a series of detailed pictures
of areas inside your body. You may receive an injection of dye. A CT
scan may show whether cancer has spread to the liver, lungs, or other
organs.
Your doctor may also use other tests (such as MRI)
to see whether the cancer has spread. Sometimes staging is not complete
until after surgery to remove the tumor.
Doctors describe colorectal cancer by the following stages:
Stage 0. The cancer is found only in the innermost
lining of the colon or rectum. Carcinoma in situ is another name for
Stage 0 colorectal cancer.
Stage I. The tumor has grown into the inner wall
of the colon or rectum. The tumor has not grown through the wall.
Stage II. The tumor extends more deeply into or through
the wall of the colon or rectum. It may have invaded nearby tissue,
but cancer cells have not spread to the lymph nodes.
Stage III. The cancer has spread to nearby lymph
nodes, but not to other parts of the body.
Stage IV. The cancer has spread to other parts of
the body, such as the liver or lungs.
Recurrence. This is cancer that has been treated
and has returned after a period of time when the cancer could not be
detected. The disease may return in the colon or rectum, or in another
part of the body.
Treatment
Read about how colon
and ractal cancer is treated.