
angina
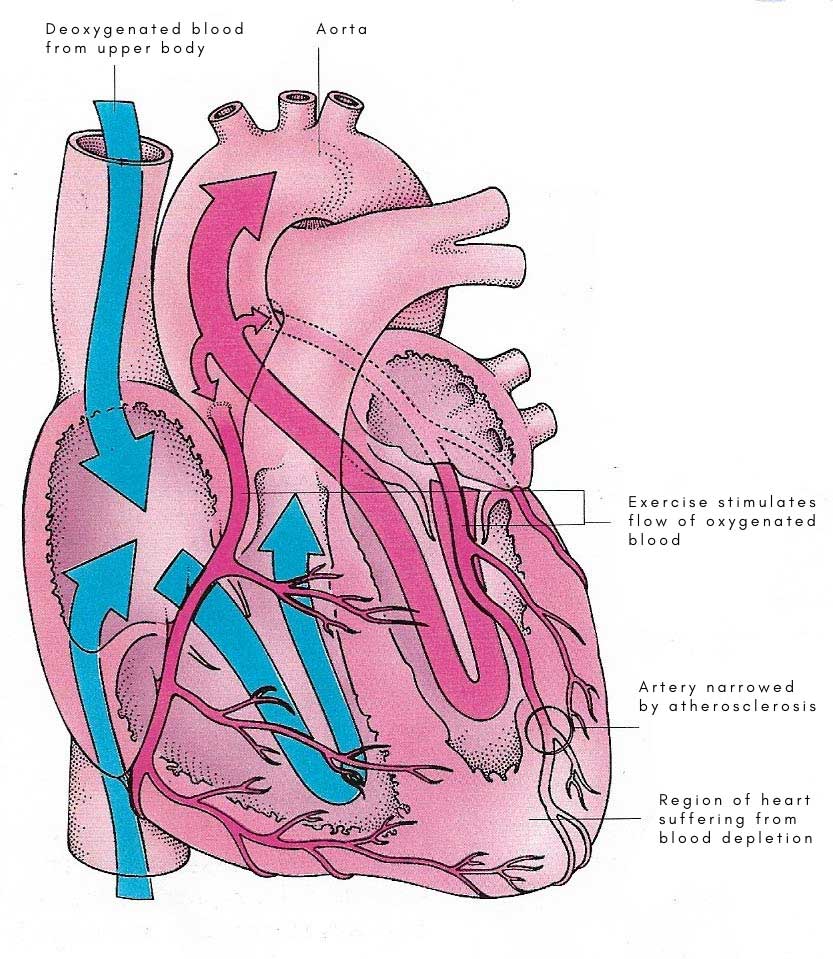
Figure 1. Angina is a sign that the heart muscle is not receiving suffiicient oygenated blood.
Figure 2. An artery with normal blood flow (A) and an artery containing plaque buildup (B). Credit: National Institutes of Health.
Angina, also called angina pectoris, is chest pain or discomfort that occurs when the muscle of the heart (see cardiac muscle) doesn't get enough blood (Fig 1). It may feel like pressure or a squeezing pain in the chest. The pain may also occur in the shoulders, arms, neck, jaw, or back. It may also feel like indigestion.
Angina is a symptom of coronary artery disease (CAD), the most common type of heart disease. CAD occurs when plaque builds up in the coronary arteries (Fig 2). This buildup of plaque is called atherosclerosis. As plaque builds up, the coronary arteries become narrow and stiff. Blood flow to the heart is reduced, which decreases the oxygen supply to the heart muscle.
Types of angina
The three types of angina are stable, unstable, and variant (Prinzmetal's). It is very important to know the differences among the types.
The pain usually goes away in a few minutes after you rest or take your angina medicine.
Stable angina is not a heart attack but makes it more likely that you will have a heart attack in the future.
Not all chest pain or discomfort is angina. Chest pain or discomfort can be caused by a heart attack, lung problems (such as an infection or a blood clot), heartburn, or a panic attack. However, all chest pain should be checked by a doctor.
Causes
Angina is caused by reduced blood flow to an area of the heart. This is most often due to coronary artery disease (CAD). Sometimes, other types of heart disease or uncontrolled high blood pressure can cause angina.
In CAD, the coronary arteries that carry oxygen-rich blood to the heart muscle are narrowed due to the buildup of fatty deposits called plaque. This is called atherosclerosis. Some plaque is hard and stable and leads to narrowed and hardened arteries. Other plaque is soft and is more likely to break open and cause blood clots. The buildup of plaque on the inner walls of the arteries can cause angina in two ways:
Stable angina
Physical exertion is the most common cause of pain and discomfort from stable angina. Severely narrowed arteries may allow enough blood to reach the heart when the demand for oxygen is low (such as when you are sitting). But with exertion, like walking up a hill or climbing stairs, the heart works harder and needs more oxygen. Other causes include:
Unstable angina
Unstable angina is caused by blood clots that partially or totally block an artery. If plaque in an artery ruptures or breaks open, blood clots may form. This creates a larger blockage. The clot may grow large enough to completely block the artery and cause a heart attack. Blood clots may form, partly dissolve, and later form again. Chest pain can occur each time a clot blocks an artery.
Variant angina
Variant angina is caused by a spasm in a coronary artery. The spasm causes the walls of the artery to tighten. This narrows the artery, causing the blood flow to the heart to slow or stop. Variant angina may occur in people with or without CAD. Other causes of spasms in the arteries that supply the heart with blood are:
Who is at risk?
More than 6 million people in the United States have angina.
People with coronary artery disease or who have had a heart attack are more likely to have angina.
Unstable angina occurs more often in older adults.
Variant angina is rare. It accounts for only about 2% of cases of angina. People with variant angina are often younger than those with other forms of angina.
Signs and symptoms
Pain and discomfort are the main symptoms of angina. These symptoms
Some people say that angina discomfort is hard to describe or that they can't tell exactly where the pain is coming from. Symptoms such as nausea, fatigue, shortness of breath, sweating, light-headedness, or weakness may also occur.
Symptoms vary based on the type of angina.
Stable angina
The pain or discomfort:
Unstable angina
The pain or discomfort:
Variant angina
The pain or discomfort:
Chest pain that lasts longer than a few minutes and is not relieved by rest or angina medicine may mean you are having – or are about to have – a heart attack.
Diagnosis
To find out if you have angina, your doctor will:
Sometimes, your doctor can diagnose angina by noting your symptoms and how they occur. Your doctor may order one or more tests to help make a diagnosis of angina. The tests your doctor may order include:
During exercise stress testing, your blood pressure and EKG readings are monitored while you walk or run on a treadmill or pedal a bicycle. Other heart tests, such as nuclear heart scan or echocardiography (see below for more information on these tests), also can be done at the same time. These would be ordered if your doctor needs more information than the exercise stress test can provide about how well your heart is working.
If you are unable to exercise, a medicine can be injected through an intravenous line (IV) into your bloodstream to make your heart work harder and beat faster, as if you are exercising on a treadmill or bicycle. Nuclear heart scanning or echocardiography is then usually done.
During nuclear heart scanning, radioactive tracer is injected into your bloodstream, and a special camera shows the flow of blood through your heart and arteries. Echocardiography uses sound waves to show blood flow through the chambers and valves of your heart and to show the strength of your heart muscle.
Your doctor also may order two newer tests along with stress testing if more information is needed about how well your heart works. These new tests are magnetic resonance imaging (MRI) and positron emission tomography (PET) scanning of the heart. MRI shows detailed images of the structures and beating of your heart, which may help your doctor better assess if parts of your heart are weak or damaged. PET scanning shows the level of chemical activity in different areas of your heart. This can help your doctor determine if enough blood is flowing to the areas of your heart. A PET scan can show decreased blood flow caused by disease or damaged muscles that may not be detected by other scanning methods.
There are different types of nuclear heart scans. Most scans have two phases – taking pictures of the heart at rest and while it is beating faster (called a stress test), although sometimes only a rest scan is done. Many heart problems show up more clearly when your heart is stressed than when it is at rest. By comparing the nuclear heart scan of your heart at rest to your heart at "stress," your doctor can determine if your heart is functioning normally or not.
Your doctor may also order blood tests, such as:
Treatment
Treatment for angina includes lifestyle changes, medicine, special procedures, and cardiac rehabilitation. The main goals of treatment are to:
Lifestyle changes and medicine may be the only treatments needed if your symptoms are mild and are not getting worse. Unstable angina is an emergency condition that requires treatment in the hospital.
Lifestyle changes
The first thing that you need to do is change your living habits to avoid bringing on an episode of angina.
You can also make other lifestyle changes, for example:
Medications
Nitrates are the most commonly used medicines to treat angina. Fast-acting preparations are taken when angina occurs or is expected to occur. Nitrates relax and widen blood vessels, allowing more blood to flow to the heart while reducing its workload.
You can use nitrates in different forms to:
People who have angina may also use:
Platelets are small blood cells that circulate through your blood vessels and help stop bleeding by sticking together to seal small cuts or breaks in tiny blood vessels. Antiplatelet medicines may not be appropriate for some people because they increase the risk of bleeding. Discuss the benefits and risks with your doctor before starting therapy with aspirin or the other antiplatelet medicines.
Special procedures
When medicines and other treatments do not control angina, special (invasive) procedures may be needed. Two commonly used procedures are:
Cardiac rehabilitation
Your doctor may prescribe cardiac rehabilitation (rehab) for angina or after bypass surgery, angioplasty, or a heart attack.
The cardiac rehab team may include:
Rehab has two parts:
Prevention
You can prevent or lower your risk for heart disease and angina by making lifestyle changes and getting treatment for related conditions.
Make lifestyle changes
You can prevent or lower your risk for angina and heart disease by making healthy lifestyle choices:
Treat related conditions
In addition to making lifestyle changes, you can help prevent angina and heart disease by treating related conditions, such as:
Living with angina
Angina is not a heart attack, but it does mean that you are at greater risk of having a heart attack than someone who does not have angina. The risk is even higher if you have unstable angina. For these reasons, it is important that you know:
Know the pattern of your angina
Stable angina usually occurs in a pattern. You should know:
After several episodes, you will learn to recognize when you are having angina. It is important for you to notice if the pattern starts to change. Changes in the pattern to look for may include:
These changes in the pattern may be a sign that your symptoms are getting worse or becoming unstable. You should seek medical attention. Unstable angina suggests that you are at high risk for a heart attack very soon.
Know your medicines
You should know what medicines you are taking, the purpose of each, how and when to take them, and possible side effects. It is very important that you know exactly when and how to take fast-acting nitroglycerin or other nitrates to relieve chest pain. They should be taken:
Long-acting nitrate preparations should be used regularly as prescribed by your doctor.
Men with impotence (erectile dysfunction) who take sildenafil (Viagra) should talk with their doctor. Taking sildenafil and nitroglycerin or other nitrates within 24 hours of each other can cause serious problems.
Ask your doctor about your other medicines. Also, see the Treatment section to read descriptions of the medicines that you are taking.
Know how to control your angina
After several episodes, you will know the level of activity, stress, and other things that can bring on your angina. By knowing this, you can take steps to prevent or lessen the severity of episodes.
Know the limits of your physical activity
Most people with stable angina can continue their normal activities. This includes work, hobbies, and sexual relations. However, if you engage in very strenuous activity or have a stressful job, you may need to discuss this with your doctor.
Know how and when to seek medical attention
If you have angina, you are at high risk of having a heart attack. Therefore, it is very important that you and your family know how and when to seek medical attention. Talk to your doctor about making an emergency action plan. The plan should include:
Be sure to discuss your emergency plan with your family members. Take action quickly if your chest pain becomes severe, lasts longer, or is not relieved by rest or medicine.
Sometimes, it may be difficult to tell the difference between unstable angina and a heart attack. Most heart attack victims wait 2 hours or more after their symptoms begin before they seek medical help. This delay can result in death or lasting heart damage.

