
stent
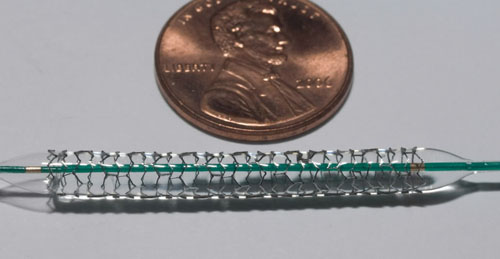
Figure 1. Stent manufactured by Boston Scientific.
Figure 2. Coronary artery stent replacement . The coronary artery is located on the surface of the heart. Fiig A shows the deflated balloon catheter and closed stent inserted into the narrowed coronary artery. The insert image on Fig A shows a cross-section of the artery with the inserted balloon catheter and closed stent. In `fig B, the balloon is inflated, expanding the stent and compressing the plaque to restore the size of the artery. Fig C shows normal blood flow restored in the stent-widened artery. The insert image on Fig C shows a cross-section of the compressed plaque and stent-widened artery.
Figure 3. Restenosis of a stent-widened coronary artery,
The coronary artery is located on the surface of the heart. In Fig
A, the expanded stent compresses plaque, allowing normal blood flow.
The inset image on Fig A shows a cross-section of the compressed
plaque and stent-widened artery. In Fig B, over time, the plaque
grows through and around the stent, causing a partial blockage and
abnormal blood flow. The inset image on Fig B shows a cross-section
of the growth of the plaque around the stent.
A stent is a small mesh-wire tube that is used to prop open a narrowed or weakened artery in the body (Figure 1).
A person may have a stent placed in an artery as part of a procedure called angioplasty. Angioplasty can restore blood flow through narrowed or blocked arteries. Stents help prevent arteries from becoming narrowed or blocked again in the months or years after treatment with angioplasty. A person may also have a stent placed in a weakened artery to improve blood flow and to help prevent the artery from bursting.
Stents are usually made of metal mesh, but sometimes they're made of fabric. Fabric stents, also called stent grafts, are used in larger arteries. Some stents are coated with medicines that are slowly and continuously released into the artery. These medicines help prevent the artery from becoming blocked again.
How are stents used?
Stents for arteries in the heart
With age and some health conditions, the inside openings of the coronary arteries (arteries of the heart) tend to narrow due to deposits of a fatty substance called plaque. High cholesterol, diabetes, and smoking can cause the arteries to narrow. This narrowing of the coronary arteries can cause angina (chest pain) or lead to heart attack.
During angioplasty, doctors use an expanding balloon inside the artery to compress the plaque and widen the passageway. The result is improved blood flow to the heart and a decreased chance of heart attack.
Unless an artery is too small, doctors usually place a stent in the treated portion of the artery during angioplasty. The stent supports the inner artery wall and reduces the chance of the artery closing up again. A stent also can keep an artery open that was torn or injured during angioplasty.
When stents are placed in coronary arteries, there's a 1 in 5 chance that the arteries will close in the first 6 months after angioplasty. When stents aren't used, the risk of the arteries closing can be twice as high.
Stents for the carotid arteries in the neck
Both the right and left sides of the neck have blood vessels called carotid arteries. These arteries carry blood from the heart to the brain. Carotid arteries can become narrowed by plaque. These plaque deposits limit blood flow to the brain and increase a person's risk for stroke. The chance of developing plaque in the carotid arteries increases with age, and may increase if the person smokes.
A new procedure uses stents to help keep the carotid arteries fully open after they're widened with angioplasty. Not all hospitals offer this procedure. How effective it is long term is still not known.
Stents for other arteries
The arteries in the kidneys also can become narrowed. This reduces blood flow to the kidneys, which can affect their ability to control blood pressure. This can cause severe high blood pressure.
The arteries in the arms and legs also can narrow with plaque over time. This narrowing can cause pain and cramping in the affected limbs. If the narrowing is severe, it can completely cut off the blood flow to a limb, which could require surgical treatment.
To relieve these problems, doctors may perform angioplasty on the narrowed kidney, arm, or leg arteries. This procedure often is followed by placing a stent in the treated artery. The stent helps keep the artery fully open.
Stents for the aorta in the abdomen or chest
The major artery coming out of the heart and supplying blood to the body is called the aorta. The aorta travels through the chest and then down into the abdomen. Over time, some areas of the walls of the aorta can become weak. These weakened areas can cause a bulge in the artery called an aneurysm.
An aorta with an aneurysm can burst, leading to potentially deadly internal bleeding. When aneurysms occur, they are usually in the part of the aorta in the abdomen. To help avoid a burst, doctors place a fabric stent in the weakened area of the abdominal aorta. The stent creates a stronger inner lining for the artery.
Aneurysms also can develop in the part of the aorta in the chest. These aneurysms also can be treated with stents. But this new use of stents is not offered by all hospitals, and how effective it is long term is still not known.
Stents to close off aortic tears
Another problem that can develop in the aorta is a tear in the inside wall. Blood can be forced into this tear, causing it to widen and eventually block blood flow through the artery or burst. When this occurs, it's usually in the part of the aorta that's in the chest.
Fabric stents are being developed and used experimentally to prevent aortic dissection by stopping blood from flowing into the tear. Tears in the aorta reduce blood flow to the tissues the aorta serves. A fabric stent placed within the torn area of the artery can help restore normal blood flow and reduce the risk of a burst aorta. Stents to treat aortic tears are still being researched. Only a few hospitals offer this procedure.
How are stents placed?
To place a stent, a small opening is made in a blood vessel in the groin (upper thigh), arm, or neck (Figure 2). Through this opening, a flexible, plastic tube (catheter) is threaded with a deflated balloon on the end. A stent may be placed around the deflated balloon. The tip of the catheter is threaded up to the narrowed artery section or to the aneurysm or aortic tear site. Special X-ray movies are taken of the tube as it is threaded up into the blood vessel. These movies help the doctor position the catheter.
For arteries narrowed by plaque
Once the tube is in the area of the artery that needs treatment:
A very narrow artery, or one that is difficult to reach with the catheter,
may require more steps to place a stent. This type of artery usually is
first expanded by inflating a small balloon. The balloon is then removed
and replaced by another larger balloon with the collapsed stent around it.
At this point, the doctor can follow the standard practice of compressing
the plaque and placing the stent.
When angioplasty and stent placement are performed on carotid arteries, a special filter device is used. The filter helps keep blood clots and loose pieces of plaque from passing into the bloodstream and brain during the procedure.
For aortic aneurysms
Placing a stent to treat an aneurysm in an artery is slightly different than treating an artery narrowed by plaque. The stent used to treat an aneurysm is made out of pleated fabric, often with one or more tiny hooks.
Once the catheter is positioned at the aneurysm site, the stent is threaded through the tube to the area that needs treatment. Then, a balloon is placed inside the stent. The balloon is inflated to expand the stent and have it fit tight against the artery wall. The hooks on the stent latch on to the artery wall to anchor the stent. The balloon and catheter and then removed, leaving the fabric stent behind.
The stent creates a new inner lining for that portion of the artery. Cells in the artery eventually grow to cover the fabric and create an inner layer that resembles what's normally seen inside a blood vessel.
Before a stent procedure
Most stent procedures require an overnight stay in the hospital and someone to take the patient home. A doctor can advise:
The should be told doctor if the patient has diabetes, kidney disease, or other conditions that may require taking extra steps during or after the procedure to avoid complications.
During a stent procedure
For arteries narrowed by plaque
This procedure usually takes a few hours.
Before the procedure starts, the patient will be given medicine to help him or her relax. The patient will be on his or her back and awake during the procedure and able to follow the doctor's instructions. The area where the catheter is inserted will be numbed and the patient will feel the doctor threading the catheter, balloon, or stent inside the artery. Some pain may be felt when the balloon is expanded to push the stent into place.
For aortic aneurysms
This procedure takes a few hours. It usually requires a 2- to 3-day stay in the hospital.
Before the procedure, a medicine is administered to help the patient relax. If a stent is placed in the abdominal portion of the aorta, the patient may be given a regional anesthetic. This will make the patient numb from the area of the stent placement down, but it will allow the patient to be awake during the procedure. If a stent is placed in the chest portion of the aorta, usually a general anesthetic will be used.
Once the patient is numbed or asleep, a small incision will be made in your groin (upper thigh). A catheter will be inserted into the blood vessel through this cut. Sometimes, two cuts (one above each leg) are needed to place fabric stents that come in two parts. The patient will not feel the threading of the catheter, balloon, or stent into the artery.
After a stent procedure
Recovery
After either type of stent procedure (for arteries narrowed by plaque or aortic aneurysm), once the stent has been placed and the balloon and catheter have been removed, the tube insertion site will be bandaged. A small sandbag or other type of weight may be put on top of the bandage to apply pressure to help prevent bleeding. The patient will recover in a special care area where his or her movement will be limited.
While the patient is in recovery, a nurse will check the patient's heart rate and blood pressure regularly. The nurse also will see if there's any bleeding from the insertion site. Eventually, a small bruise and sometimes a small, hard "knot" will appear at the insertion site. This area may feel sore or tender for about a week.
The patient should inform the doctor if he or she:
Common precautions after a stent procedure
After a stent procedure, the patient may be put on blood-thinning or anticlotting medicines for at least a few months. These medicines help prevent the development of blood clots in the stent. If the stent is coated with medicine, the patient may be advised to take aspirin and an anticlotting medicine for months to years to lower the risk of blood clots.
Vigorous exercise and heavy lifting should be avoided for a short time after the procedure. A doctor will discuss with the patient when he or she can resume normal activities.
If a patient has a metal stent placed, he or she should not have a magnetic resonance imaging (MRI) test within the first couple of months after the procedure. Metal detectors used in airports and other screening areas don't affect stents.
If a patient has an aortic fabric stent, the patient will probably be recommended to have followup imaging tests (for example, X-ray) within the first year of having the procedure, and yearly imaging tests after that.
Risks
Risks related to angioplasty
Any medical procedure has risks, but major complications from angioplasty are rare. The most common risks from angioplasty include:
Another common problem after angioplasty is too much tissue growth within the treated portion of the artery. This can cause the artery to narrow or close again, which is called restenosis (Figure 3). This problem is often avoided with the use of newer stents coated with medicines that help prevent too much tissue growth. Treating the tissue around the stent with radiation also can prevent tissue growth. For this procedure, the doctor puts a wire through a catheter to where the stent is placed. The wire releases radiation and stops cells around the stent from growing and blocking the artery.
Risks related to stent
About 1 to 2 percent of people with a stented artery develop a blood clot at the stent site. Blood clots can cause heart attacks, strokes, or other serious problems. The risk of blood clots is greatest during the first few months after the stent is placed in the artery. Patients are usually put on blood-thinning or anticlotting medicines for at least a few months after having a stent procedure to prevent blood clots.
Stents coated with medicine (drug-releasing stents), which are often used to keep clogged heart arteries open, may increase a patient's risk for potentially dangerous blood clots. But an expert Food and Drug Administration panel found no conclusive evidence that these stents increase the chances of having a heart attack or dying, if used as recommended. Patients with drug-releasing stents are usually advised to take aspirin and an anticlotting drug, such as clopidogrel, for months to years to lower the risk of blood clots.
Risks related to aortic stents in the abdomen
Whenever an aneurysm in the abdomen region of the aorta is repaired with either surgery or with a fabric stent, few rare but serious complications can occur, including:
Another possible complication is the fabric stent moving further down the aorta. This sometimes happens years after the stent is first placed. Such stent movement may require a doctor to place another fabric stent in the area of the aneurysm.

