
aplastic anemia
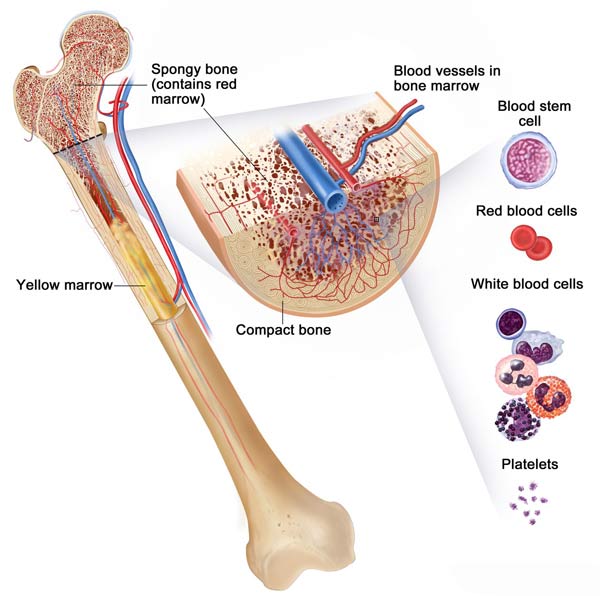
Bone anatomy
Aplastic anemia is a rare and serious blood disorder in which bone marrow stops making enough new blood cells. Bone marrow – the spongy material inside bones – makes new blood cells called stem cells. Stem cells normally develop into three main types of blood cells: red blood cells (erythrocytes), white blood cells (leukocytes), and platelets. Each type of blood cell has its own functions in the body.
It is normal for blood cells to die. The lifespan of red blood cells is about 120 days. White blood cells live less than 1 day. Platelets live about 6 days. As a result, bone marrow must constantly make new blood cells. The term "anemia" is most often used to mean a condition in which a person's number of red blood cells is too low or their red blood cells do not carry enough hemoglobin. However, in aplastic anemia, normal production of all blood cells – red cells, white cells, and platelets – slows or stops. This is because the stem cells have been damaged. The cause of this damage is often unknown.
Effects of aplastic anemia on the body
A shortage of any one of the three main types of blood cells will have an effect on the body. In aplastic anemia, however, the body must cope with a shortage of all three types of blood cells. Severe aplastic anemia that is not treated promptly can be fatal.
The effect on the body of a shortage of each type of blood cell is described below:
Important general information
Aplastic anemia is a rare condition. In the United States, about 500–1,000 people develop this type of anemia each year. It is two to three times more common in Asian countries.
The two main types of aplastic anemia are acquired and hereditary. Acquired means a person develops the condition during his or her lifetime. Hereditary means a person is born with the condition. Acquired aplastic anemia is the most common type, and it is sometimes a temporary condition. It can be triggered by exposure to:
However, the cause of acquired aplastic anemia is often not known.
Hereditary aplastic anemia is rare. It occurs with some inherited conditions,
such as Fanconi anemia.
Severity of aplastic anemia
Aplastic anemia can begin suddenly or develop slowly. It tends to get worse over time, except when a cause can be found and removed. Its severity ranges from mild to very severe.
Although aplastic anemia is not cancer, the treatments for it are similar to those used for some types of cancer. Treatments include blood transfusions and bone marrow transplants. Treatments also include medicines to suppress the immune system, stimulate the bone marrow, and treat infections.
Outlook
Many people with aplastic anemia can be treated successfully if they have
prompt and appropriate treatment. Some people with aplastic anemia can be
cured with a bone marrow transplant.
Causes
Aplastic anemia is caused by damage to stem cells in the bone marrow. Stem cells normally develop into three types of blood cells: red blood cells, white blood cells, and platelets. When stem cells are damaged, they do not grow into healthy blood cells.
In more than half of people with aplastic anemia, the cause of the damage to stem cells is unknown. Some research suggests that stem cell damage may occur because the body's immune system attacks its own cells by mistake.
Causes of acquired aplastic anemia
The cause of acquired aplastic anemia has been linked to outside agents, as well as to diseases. Outside agents include toxins such as pesticides, arsenic, and benzene; radiation and chemotherapy used to treat cancer; and medicines such as chloromycetin (chloramphenicol), an antibiotic now rarely used in the United States. Infectious diseases also can cause aplastic anemia. Some of these diseases are hepatitis, Epstein-Barr virus, cytomegalovirus, parvovirus B19, and HIV. Autoimmune diseases, such as lupus and rheumatoid arthritis, also can cause this condition.
Causes of hereditary aplastic anemia
Some inherited genetic disorders can lead to aplastic anemia. These include Fanconi anemia, Shwachman-Diamond syndrome, and dyskeratosis congenita.
Who is at risk?
Aplastic anemia is a rare condition. In the United States, about 500–1,000 people develop this type of anemia each year. It is two to three times more common in Asian countries.
People of all ages can develop aplastic anemia. Men and women are equally likely to have it. It is most common in adolescents and young adults as well as the elderly.
Aplastic anemia is more likely to develop in people who:
Signs and symptoms
Most of the signs and symptoms of aplastic anemia are caused by low numbers of each of the three main types of blood cells – red blood cells, white blood cells, and platelets. Other signs and symptoms are not linked to a shortage of any particular blood cell type.
Too few red blood cells
The most common symptom of a low red blood cell count is low energy and feeling tired. This is caused by lack of enough hemoglobin, an iron-rich protein contained in red blood cells that carries oxygen to the body. A lack of enough oxygen in the blood can cause people to feel short of breath and dizzy, especially when standing up. Since the heart must work harder to circulate the reduced amount of oxygen, symptoms also can include a rapid or irregular heartbeat or an extra or unusual sound heard during the heartbeat (heart murmur).
The hemoglobin in red blood cells gives blood its red color. Lack of hemoglobin due to a low red blood cell count can lead to pale skin, gums, and nail beds.
Too few white blood cells
White blood cells help fight infections. Signs and symptoms of a low white blood cell count are fevers, frequent infections which can be severe, and flu-like illnesses that linger.
Too few platelets
People who do not have enough platelets tend to bruise and bleed easily, and the bleeding may be hard to stop. Common types of bleeding related to too few platelets include nosebleeds, bleeding gums, pinpoint red bleeding spots on the skin, and blood in the stool. Women also may have heavy menstrual bleeding.
Other signs and symptoms
Aplastic anemia can cause other signs and symptoms as well. Some occur in the area of the head. These signs and symptoms include headache, tender sinuses, and white patches in the mouth (oral thrush). Other signs and symptoms are nausea and rash. A person with aplastic anemia also may have an enlarged spleen or liver.
Paroxysmal nocturnal hemoglobinuria
About one-third of people with aplastic anemia have a condition called paroxysmal nocturnal hemoglobinuria (PNH). This is a disorder of the red blood cells. Most people with PNH don't have any signs or symptoms. If they do occur, they may include:
Some people have PNH first and then develop aplastic anemia. But this process can also happen in reverse. People may have aplastic anemia first and then develop PNH later.
Diagnosis
Aplastic anemia is diagnosed using a medical and family history, a physical exam, and tests to discover the type and cause of anemia. Your doctor can use these methods to find out how severe the anemia is and to decide the appropriate treatment.
Specialists involved
A person with suspected aplastic anemia may be referred to a hematologist (an expert in treating blood conditions).
Medical and family history
During a medical history, your doctor may ask detailed questions about many kinds of symptoms. He or she may ask if you have ever had problems with anemia, had an illness or condition that could cause anemia, or been exposed to drugs, chemicals, or radiation. The doctor will ask about medicines you are taking to see if they might be a cause of the anemia. The doctor will also ask if your family members have ever had any kind of anemia.
Physical exam
Your doctor will do a physical exam to see how severe the anemia is and to check for its possible causes. This exam may include:
Diagnostic tests and procedures
Several tests of the blood and bone marrow may be used to diagnose aplastic anemia. The reasons for testing are to:
Complete blood count
Usually, the first test used to diagnose anemia is a complete blood count (CBC). The CBC tells a number of things about a person's blood, including:
The normal range of these levels may be lower in certain racial and ethnic populations. Your doctor can explain your individual test results.
The CBC also checks:
Reticulocyte count
This test measures the number of new red blood cells in the blood. It helps doctors find out whether bone marrow is producing red blood cells at the proper rate. A lower than average level can mean that the bone marrow is not making enough red blood cells. The reticulocyte level is low in people with aplastic anemia.
Bone marrow tests
This test looks at the bone marrow to see if it is healthy and if it is making enough blood cells. A small amount of bone marrow may be removed and examined. Removing a small bit of liquid bone marrow is called aspiration. Removing bone marrow tissue is called biopsy.
A bone marrow aspiration may be done to find what is causing the low production of blood cells. Since blood cells are formed inside the bones, doctors use a needle to remove a small amount of liquid bone marrow. The sample is then examined under a microscope to check for abnormal cells.
A bone marrow biopsy is usually done at the same time, especially if an aspiration was not productive. A small number of bone marrow cells with a small piece of bone is removed using a needle. This test checks the number and type of cells in the bone marrow. In aplastic anemia, the bone marrow has a lower than normal number of cells.
Other tests
Additional tests may be used to help diagnose aplastic anemia, including:
Treatment
Treatments for aplastic anemia include:
In rare cases, no treatment is needed.
In general, treatments for aplastic anemia can limit and prevent complications, relieve symptoms, and improve quality of life. For some, a cure may be possible. Bone marrow transplants can be a cure for those people who are eligible for a transplant. Removing a known cause of aplastic anemia (such as exposure to a toxic chemical) also can cure the disorder. Other treatments can restore blood cell counts to levels high enough so that a person can live a normal life.
Who needs treatment
People with mild or moderate aplastic anemia may not need treatment as long as the condition does not get worse. People with severe aplastic anemia need immediate medical treatment to prevent complications from the very low levels of blood cells in their bodies. People with very severe aplastic anemia need emergency medical care and hospitalization or the anemia can be fatal in a short time.
Blood transfusions
Blood transfusions are used to keep blood counts high enough in people with aplastic anemia. Healthy blood is taken from matched donors and then given to the person with aplastic anemia through an injection in a vein. Blood transfusions help relieve symptoms. They are not an effective long-term treatment.
Red blood cells
Red blood cell transfusions help relieve lack of energy, tiredness, and shortness of breath. However, if red blood cells are given often, the immune system in the body can learn to recognize these new cells, develop antibodies against them, and destroy these newly transfused cells. Also, if red blood cells are given often, the body can build up too much iron. Excess iron from transfusions can damage the heart, liver, and other organs. If this happens, treatment may be needed to remove excess iron from the body.
White blood cells
White blood cells are not routinely transfused because they live in the bloodstream for less than 1 day. However, they may be used for severe infections that are not being helped by antibiotics.
Platelets
Platelet transfusions reduce the risk of fatal bleeding. Several transfusions a month are often needed because platelets live only a few days. However, in time, the immune system will learn to recognize and destroy newly transfused platelets by making antibodies, just as it does with red blood cells.
Bone marrow transplantation
A bone marrow transplant replaces damaged stem cells in bone marrow with healthy stem cells from a donor's bone marrow. It is the best treatment choice for eligible people because it usually cures aplastic anemia.
A bone marrow transplant works best in children and young adults with severe aplastic anemia who are in good health and who have matched donors. Older people are less able to tolerate the treatments needed to prepare the body for the transplant. They also are more likely to have complications after the transplant. There are age limits for who can receive a bone marrow transplant, but they vary among hospitals.
Finding a donor
For best results, the donor's bone marrow must be a close match with the bone marrow of the person with aplastic anemia. A matched donor is found by means of a blood test that looks at proteins on the surface of body cells. These proteins are called human leukocyte antigens (HLA). The donor and the person with aplastic anemia are both tested. The HLA antigens on their cells are compared.
Bone marrow transplants work best if the donated marrow is an exact match and comes from a family member, such as a brother or sister. A person receiving bone marrow that is an exact match usually has fewer complications. Only about 20–35 percent of people with severe aplastic anemia have an HLA-matched family member to donate bone marrow.
If no matching family member is found, the search for bone marrow widens. Millions of volunteer donors are registered with the National Marrow Donor Program. Doctors will look for:
A person who is going to have a bone marrow transplant should not receive blood transfusions from close family members before the transplant. When a person receives blood transfusions, their bodies can develop antibodies against the donated blood. If a person develops antibodies against the blood of a close family member, the person would not be able to receive a bone marrow transplant from that family member.
Receiving the transplant
Bone marrow transplants are done in special units in hospitals to try to protect the person with aplastic anemia from any infections. Before the transplant, the person receives high doses of chemotherapy, radiation therapy, or both. These treatments destroy the abnormal bone marrow that is not producing blood cells.
A sample of bone marrow is taken from the donor and is given to the recipient through a vein. The donated bone marrow stem cells travel to the recipient's bone marrow and start to make healthy blood cells. If the transplant is successful, the new stem cells multiply and begin making new, healthy blood cells within 3 to 4 weeks.
Possible complications
After a bone marrow transplant, the recipient is in the hospital for weeks or months. During this time, he or she is isolated and closely watched for infections and other complications. Complications are most likely to occur in the first 100 days after a transplant. Complications include rejection of the graft and what is called graft-versus-host disease (GVHD).
To help prevent GVHD, donor marrow is sometimes treated or people may be given medicines that suppress the immune system after the transplant. Those who develop mild but acute GVHD are treated with medicines such as steroids.
Medicines to stimulate bone marrow
Manmade versions of substances that occur naturally in the body are used to stimulate the bone marrow to produce more blood cells. Bone marrow that can produce more blood cells can help a person with aplastic anemia avoid blood transfusions. An increased number of white cells can help protect a person from infection. Examples of bone marrow stimulation medicines used to treat aplastic anemia are:
Medicines to suppress the immune system
Since research suggests that aplastic anemia may occur because the body's immune system attacks its own cells by mistake, certain medicines may be used to suppress the body's immune system. They allow the bone marrow to start making blood cells again, and they help avoid the need for blood transfusions. Medicines that suppress the immune system do not cure aplastic anemia, but they can relieve its symptoms and reduce its complications.
These medicines are often used for people who are not good candidates for a bone marrow transplant or who are waiting for a bone marrow transplant.
There are three medicines – often given together – that will suppress the body's immune system:
If this treatment is successful, it may take a few months to notice the effects of these medicines. Most often, as blood counts rise, symptoms lessen. Blood counts in people who respond well to these drugs do not usually reach normal levels, but they are often high enough to allow people to take part in their normal activities. People with aplastic anemia may need to take the medicines indefinitely to keep their blood counts high enough to resume normal daily life.
Medicines that suppress the immune system can have side effects. They also may increase the risk of developing leukemia or myelodysplasia. Leukemia is a type of cancer in which the number of white blood cells increases. MDS is a condition in which the bone marrow produces too many defective blood cells.
Antibiotics
Antibiotics and antivirals are given to people with aplastic anemia to prevent and treat infections.
Living with aplastic anemia
Many people with aplastic anemia can be treated successfully and some can be cured. Most people are able to resume their normal activities after treatment. If you are being treated for aplastic anemia, it may take a long time to get a good response from your treatment. You may need repeated treatments, or you may need to try several treatments before finding one that works.
Lifelong follow-up is needed to make sure the disorder doesn't return, as well as to check for possible complications.
Ongoing health care needs
Treatment for aplastic anemia can result in side effects or complications. Your doctor can talk with you about how to cope with symptoms of aplastic anemia, side effects of treatment, and complications from treatment.
Recommended physical activity
Your doctor might discuss what type and amount of physical exercise may be helpful. For example, you may need to avoid activities that cause chest pain or shortness of breath. You may want to stay away from activities that could result in injuries and bleeding, such as contact sports.
Protection from infection
Your doctor also might discuss ways to reduce your chance of getting an infection. These ways include staying away from people who are ill, avoiding crowds, and avoiding certain kinds of foods that could expose you to bacteria (for example, uncooked food can be a source of bacteria). You may be advised to wash your hands thoroughly several times throughout the day and to care for your teeth and gums to reduce the risk of infection in your mouth or throat.
It is important to know the signs of infection, such as a fever. Call your doctor at the first sign of an infection.

